Disruptions in the City
“Disaster does not come beating the drum” This is a proverb commonly used in Nepali society. This simply means that disaster takes place/ happens all of sudden. It does not give you big signals; beating drums. Disaster does not provide you fix date and time when will it happen but you can get prepared to cope with possible disaster to have minimal impact of disasters in terms of human and other casualty and loss of properties. Disasters can be classified broadly in two types; natural disasters and man-made disasters. Sometimes a disaster is caused by nature but with human influence and called hybrid or mixed.
Our cities are not ready for an unexpected disruption such as the 2020 pandemic. COVID-19 has placed immense pressure on our healthcare system and forced organizations to dramatically change the way they operate and to co-operate in new ways. The pandemic can offer a fresh sense of urgency to resolve these issues and leave us with a system that works better and in a smarter way. And although we are aware of the limitations to prevent this type of threat, we can be more prepared to contain it whenever and wherever it hits.
Unexpected emergencies generate high pressure on demand and supply of infrastructure, logistics (transportation), and space (buildings) in cities. Disaster has multi-facet negative consequences including the disruption to the normal pattern of life, human effects such as loss of life, injury, hardship and adverse effects on health, effects on social and physical structures, deprivation of community needs such as shelter, food, clothing, etc. The cost of disaster impact is quite huge to the societies and the government. So, every government and society must be serious to manage and keep its possible consequences at minimal.
COVID-19: 2020 Pandemic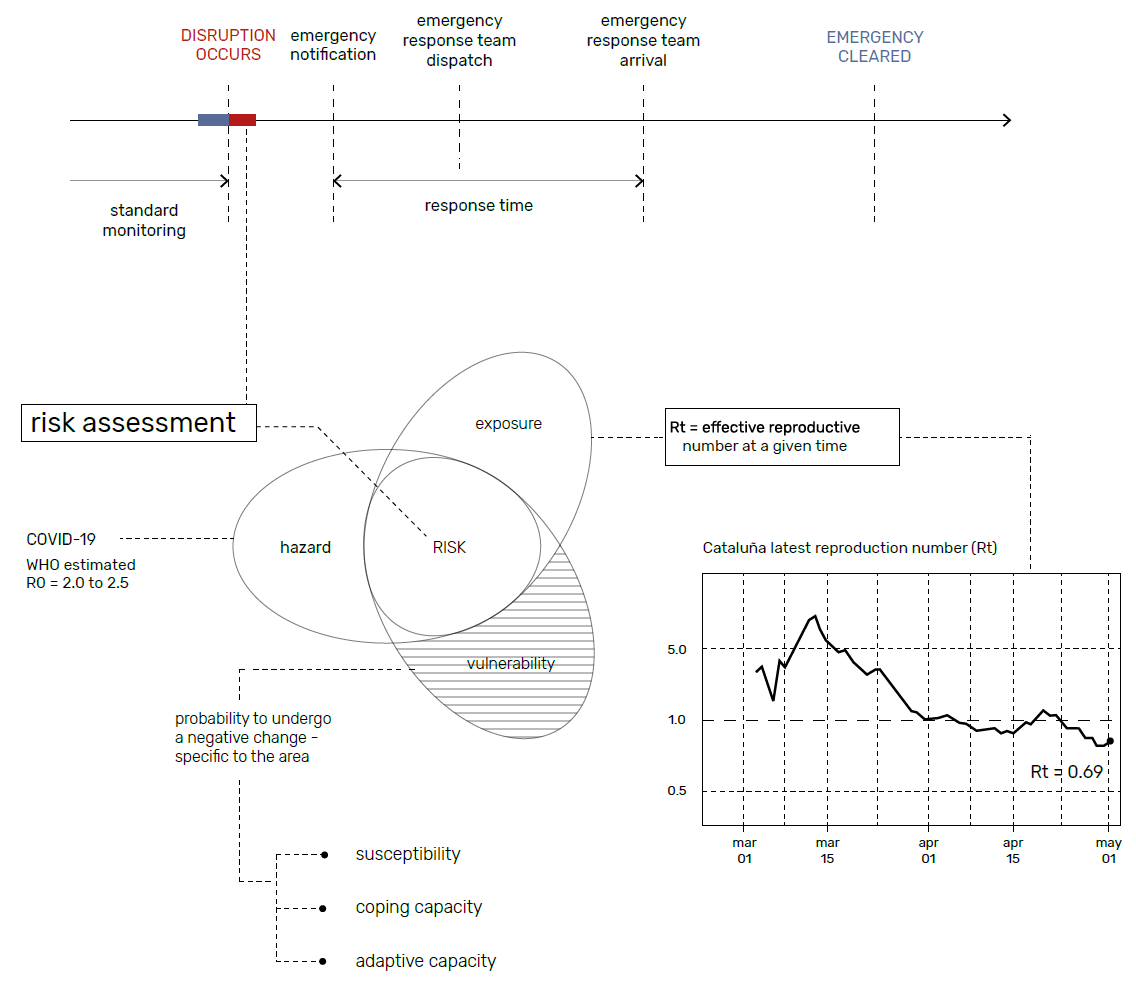
A pandemic refers to the spread of a human disease across borders and continents, in the narrower sense the spread of an infectious disease. In contrast to the epidemic, a pandemic is not locally restricted, but there can also be areas in which the disease does not affect pandemics. SARS-CoV-2 coronavirus COVID-19. Coronavirus disease(COVID-19) is an infectious disease caused by a newly discovered coronavirus. Most people infected with the COVID-19 virus will experience mild to moderate respiratory illness and recover without requiring special treatment. Older people and those with underlying medical problems like cardiovascular disease, diabetes, chronic respiratory disease, and cancer are more likely to develop serious illness.
In the case of infective disease, the urban environment has a higher risk and infection counts because of a higher population density and a higher transmission of the virus. Catalunia and Madrid have a relatively high Infection rate in comparison with other Spanish regions without urban cities with similar scales.
Reactive Pandemic Protocol
![]()
Preparedness and Resilience
There are two defining concepts embedded in the project. The first is preparedness which The United Nations and WHO defined as the ability (knowledge, capacities, and organizational systems) of governments, professional response organizations, communities, and individuals to anticipate, detect and respond effectively to, and recover from, the impact of likely, imminent or current health emergencies, hazards, events or conditions. It means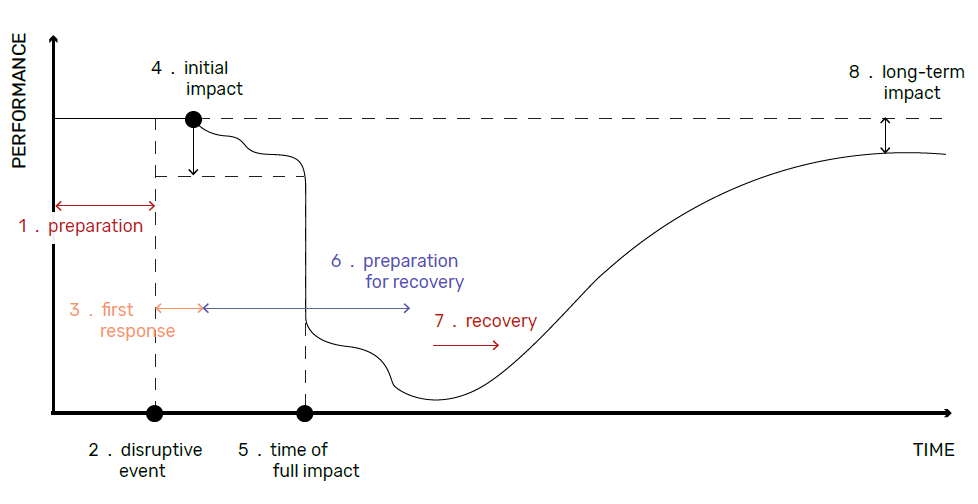 putting in place mechanisms that will allow national authorities, multilateral organizations, and relief organizations to be aware of risks and deploy staff and resources quickly once a crisis strikes. The second is resilience which describes the capacities of societies, communities, and individuals or a social-ecological system to deal with adverse consequences and the impacts of a hazard.
putting in place mechanisms that will allow national authorities, multilateral organizations, and relief organizations to be aware of risks and deploy staff and resources quickly once a crisis strikes. The second is resilience which describes the capacities of societies, communities, and individuals or a social-ecological system to deal with adverse consequences and the impacts of a hazard.
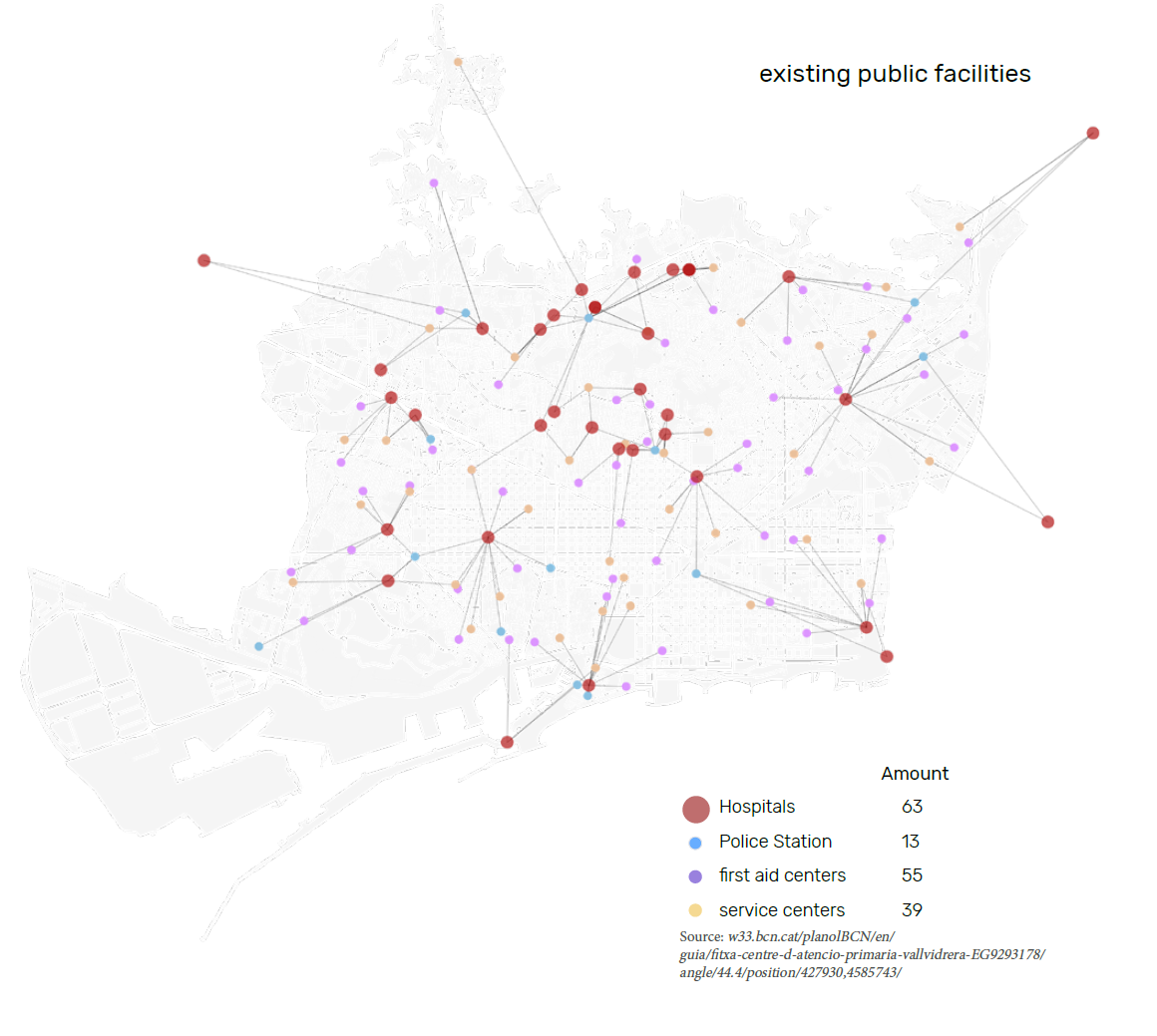
COVID-19: The Case of Barcelona
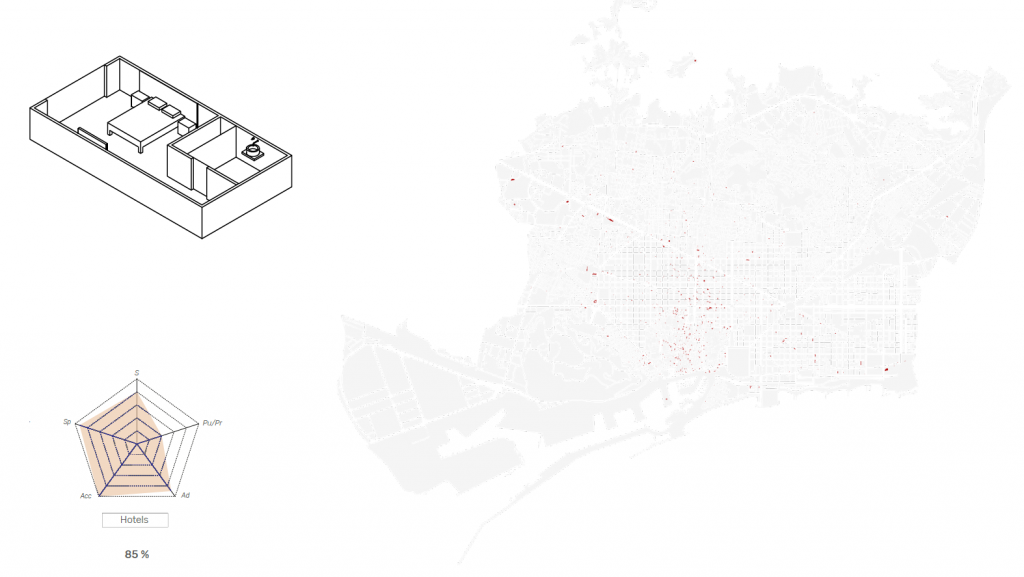
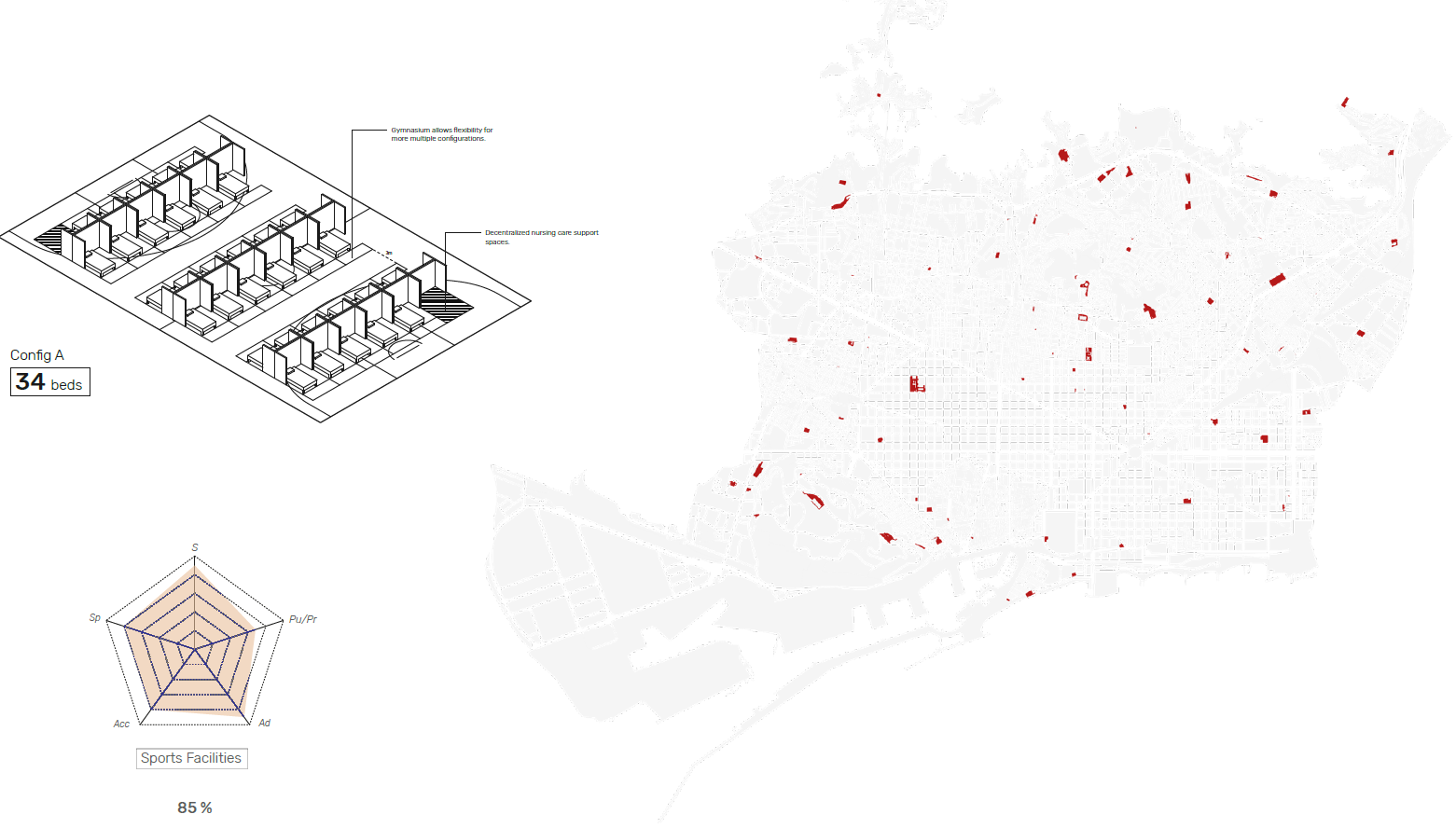
Barcelona was one of the most affected cities by Covid-19 in Spain. Existing public hospitals were especially overcapacity. It has a total number of 10, 272 hospital beds which means by a population of 5.5 Million people that the city has one bed for every 543 people. To supply the city with enough hospital beds, they were transforming dozens of public and private facilities into makeshift extensions of their hospitals. The lack of beds in health centers for such an avalanche of coronavirus patients has led authorities to resort to those in hotels and to convert large sports centers and gyms into field hospitals for hundreds of patients.
![]()
Risk Assessment
To make a risk assessment it is fundamental to analyze the pandemic’s level of hazard by its reproductive number. To conduct a more precise analysis, this data should be extracted from the specific area of study and at a given time.
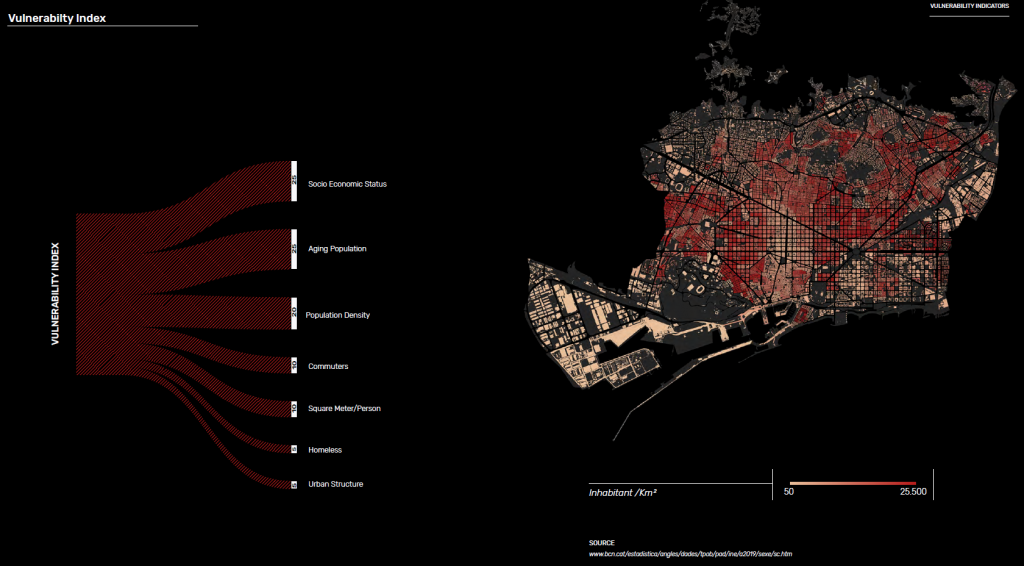
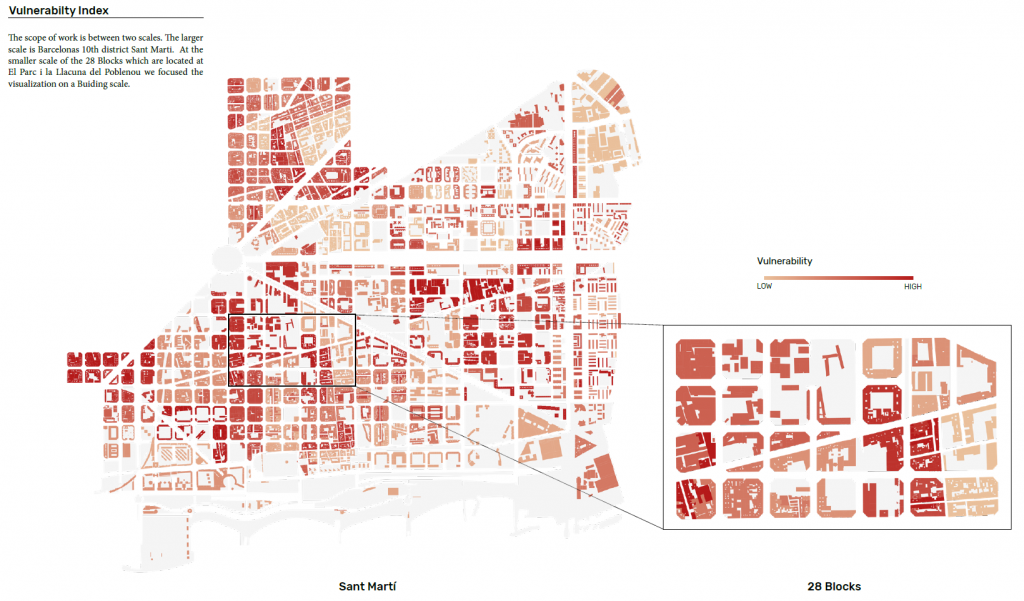
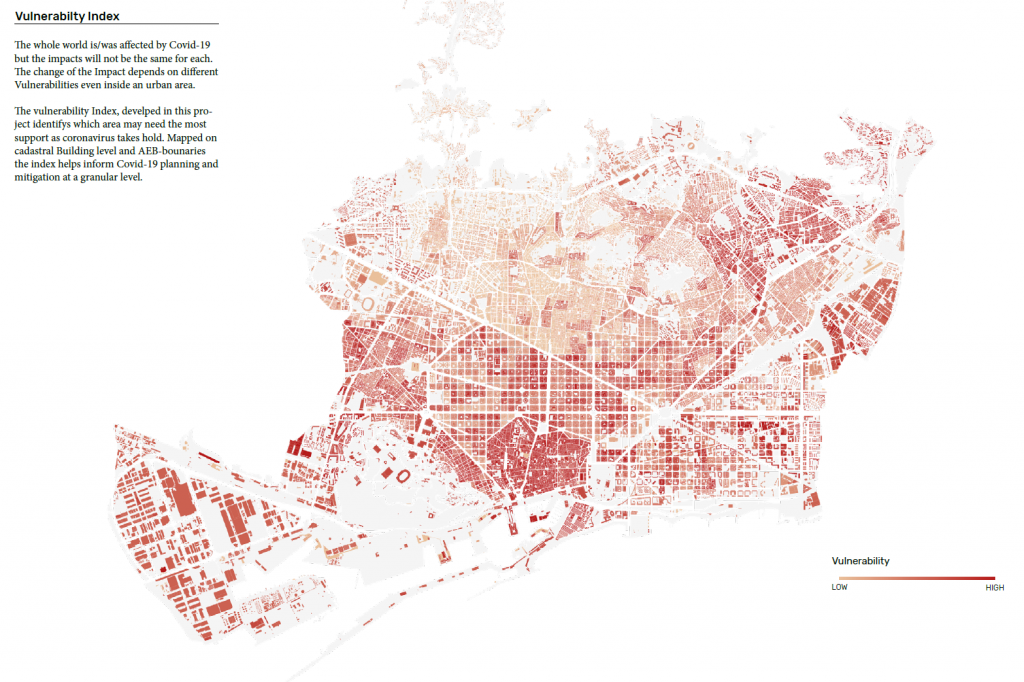
Vulnerability Index
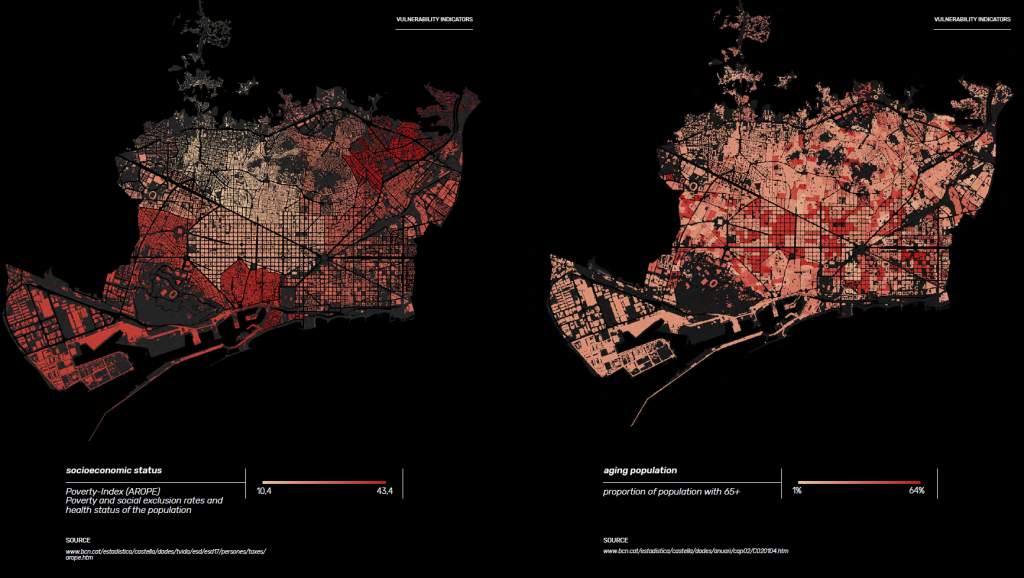
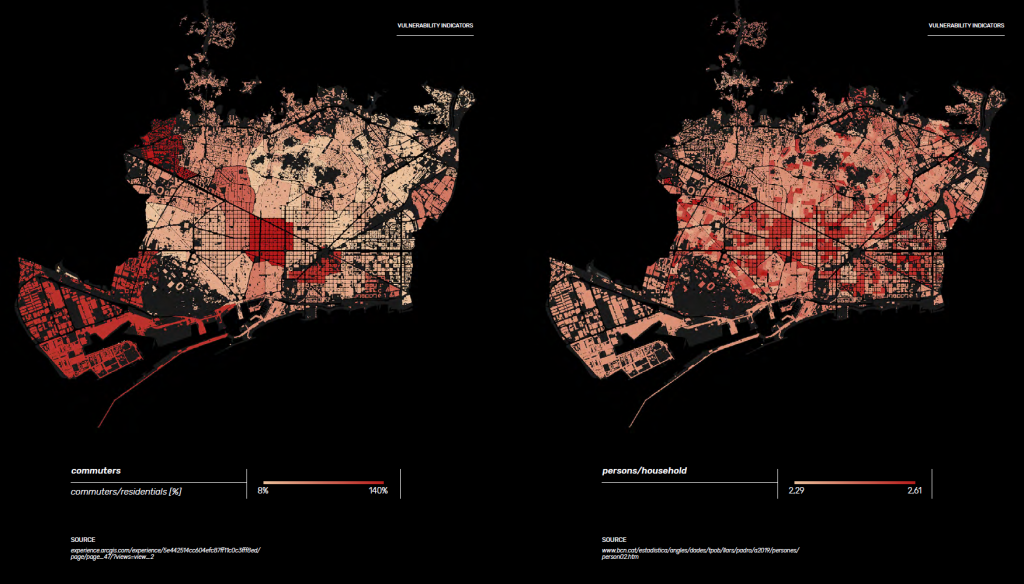
The whole world is/was affected by Covid-19 but the impacts will not be the same for each. The change of the Impact depends on different vulnerabilities even inside an urban area. The vulnerability Index, developed in this project identifies which area may need the most support as coronavirus takes hold. Mapped on a cadastral Building level and AEB-boundaries the index helps inform Covid-19 planning and mitigation at a granular level. In order to simulate the progression of the COVID-19 virus, the context in which it initially spread was analyzed. Specific vulnerabilities which may cause the increased likelihood of further spreading the infection or limit the delivery of services and resources were listed and weighted as the following: the ratio of small streets (5%), socioeconomic vulnerability (25%), population density (20%), aging population (5%), number of commuters (10%), big households (10%).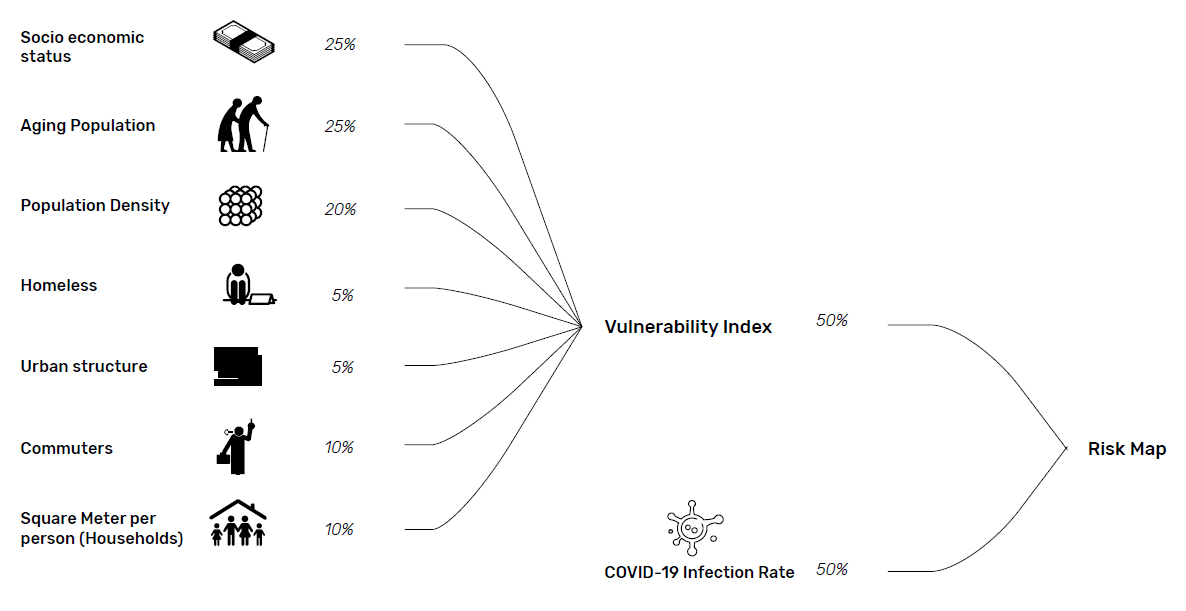
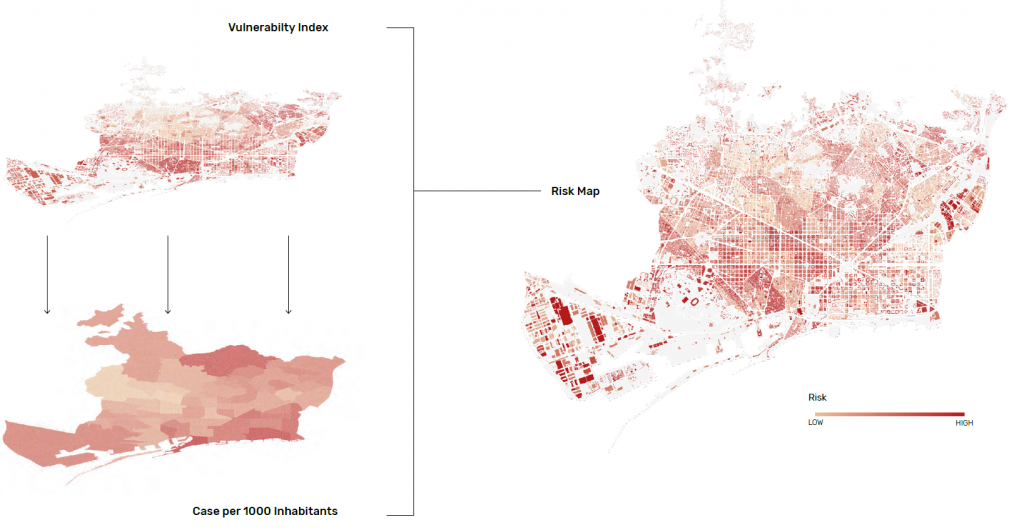
Infection Count
While the Vulnerability Index shows the inferred risk areas, the actual infection count provides validation. The infection count values are the standardized rate of positive cases per 10,000 inhabitants. The dataset uses the ABS (basic health area) boundaries which is the main territorial unit through which primary health care services are organized. These boundaries were also used for the map visualization in order to accurately reflect the infected population during the time the data was collected.
Risk Areas
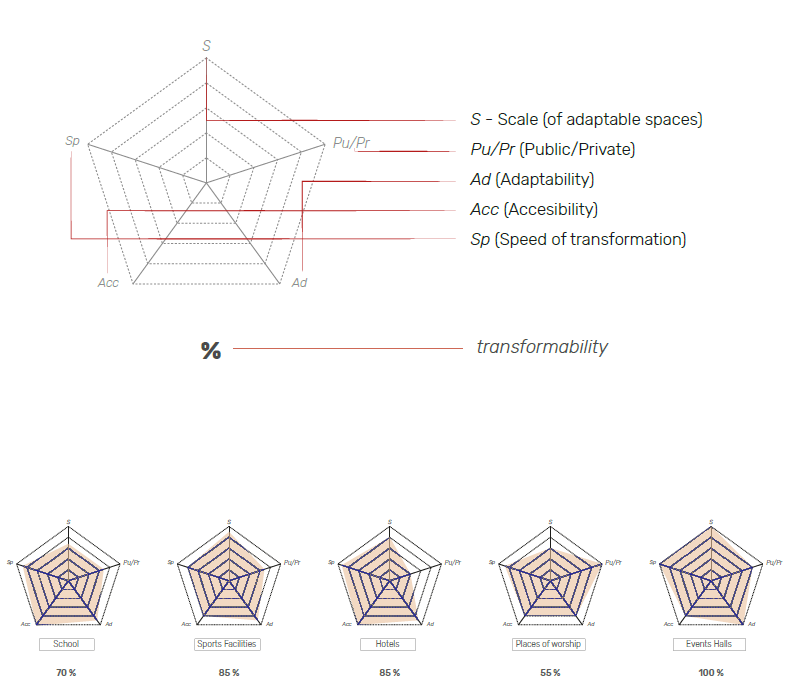
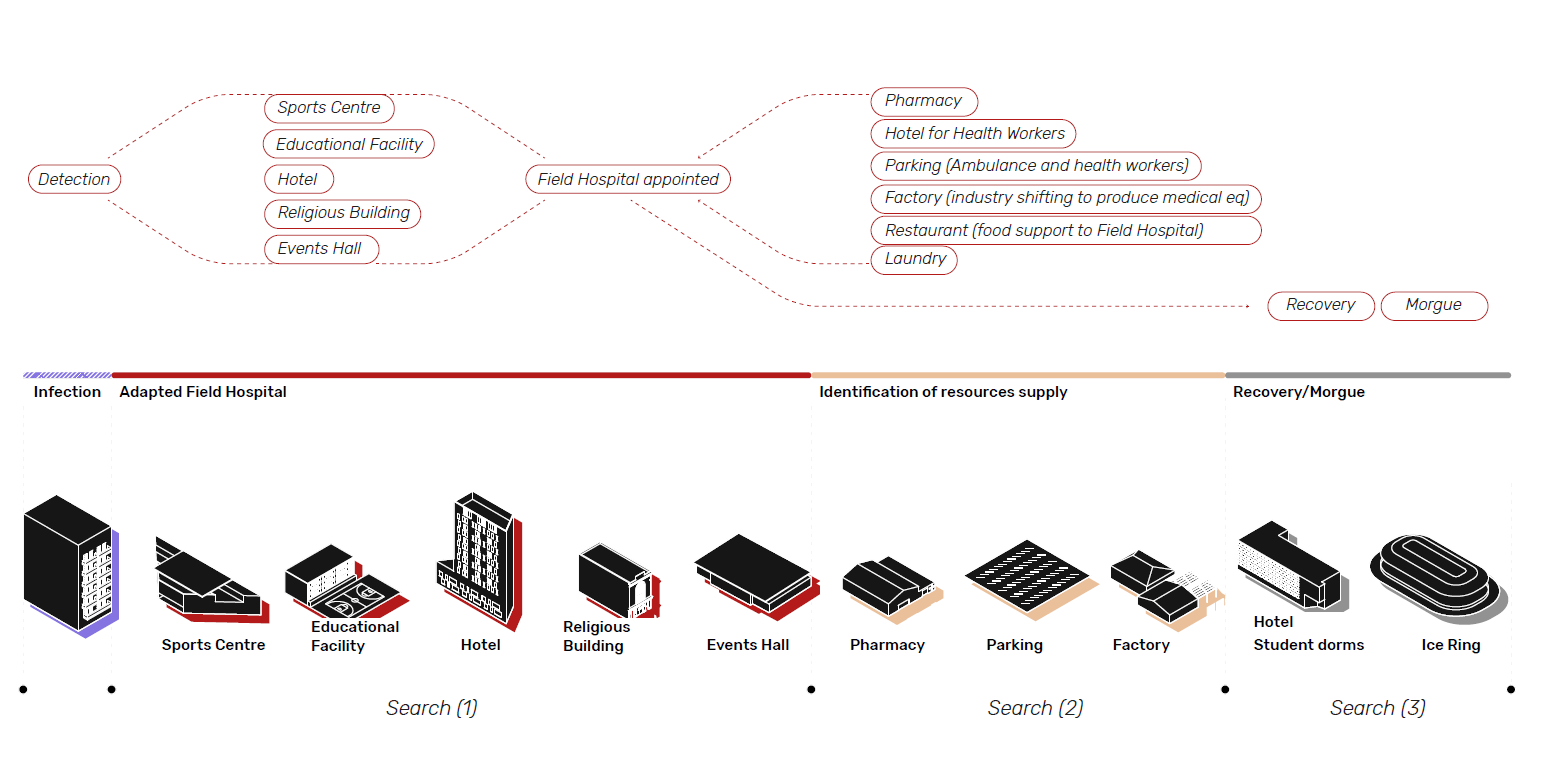
Adaptable Typologies
In order to increase the capacity of Hospital Beds for overflowing healthcare facilities, different cities and countries all over the world acted in different ways and give us an idea of the possibilities.
Law 4/1981 ART. 11/section c
Measures involved in the state of alarm can include limiting the movement of people or vehicles at specific times, temporary confiscations of goods, intervening in or temporarily taking over industries, workshops, factories and any sort of premises except for homes, limiting or rationing the use of services or the consumption of basic necessities, and issuing the necessary orders to ensure market supplies.
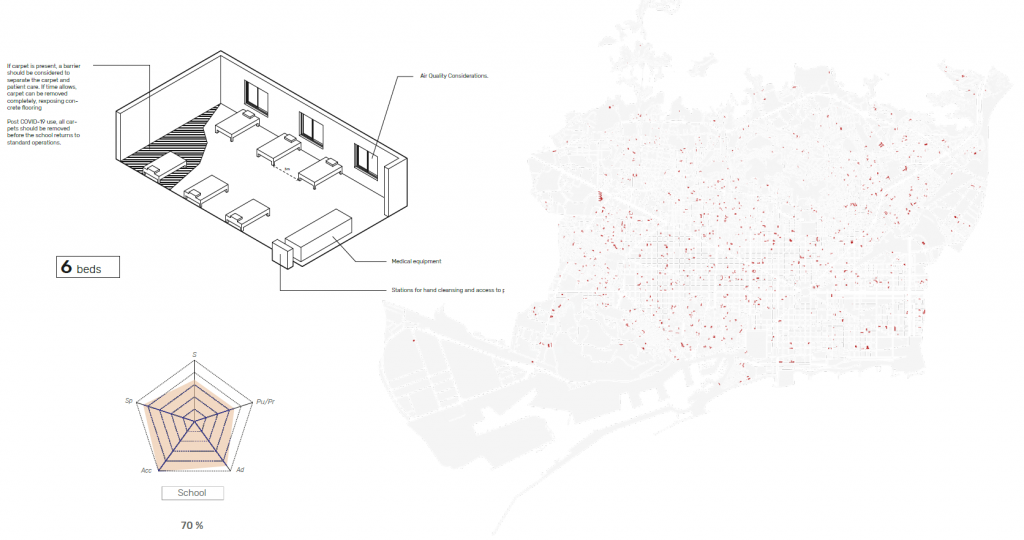
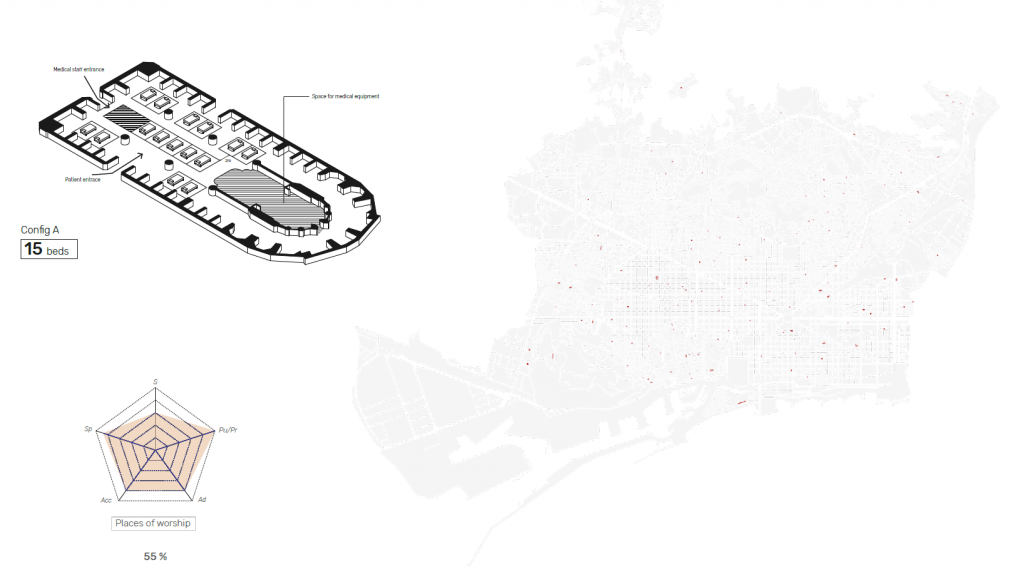
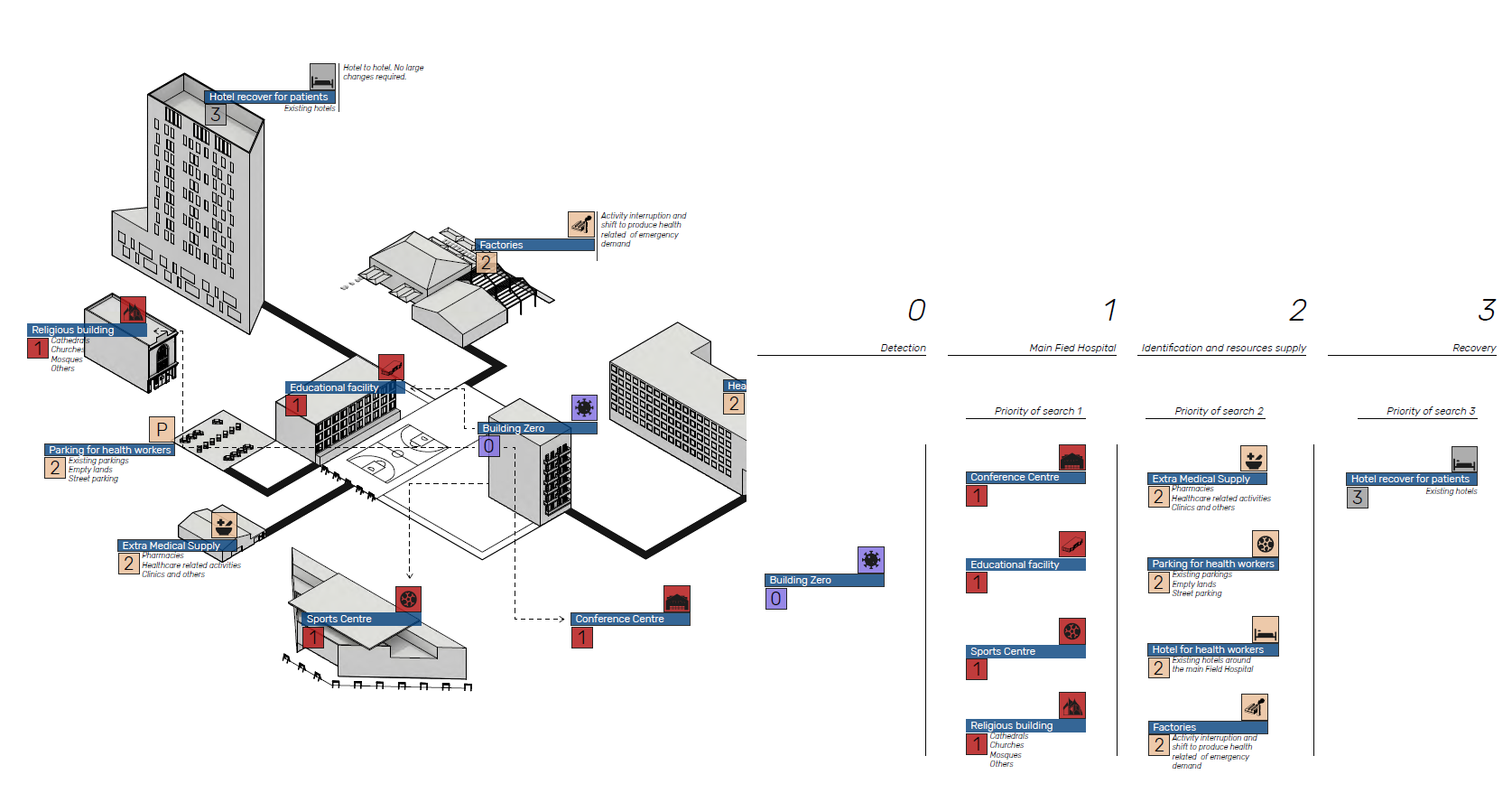
Reprogramming Buildings
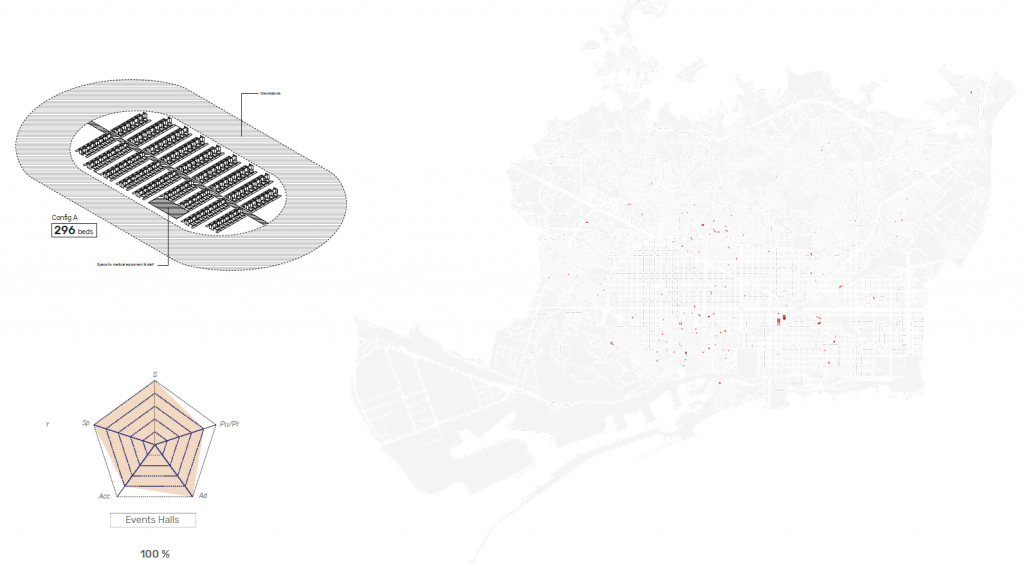
The Building Network consists of an adapted Field Hospital and different Support Facilities. Based on different configurations variations of Building Networks depending on selected adaptable typologies configuration.
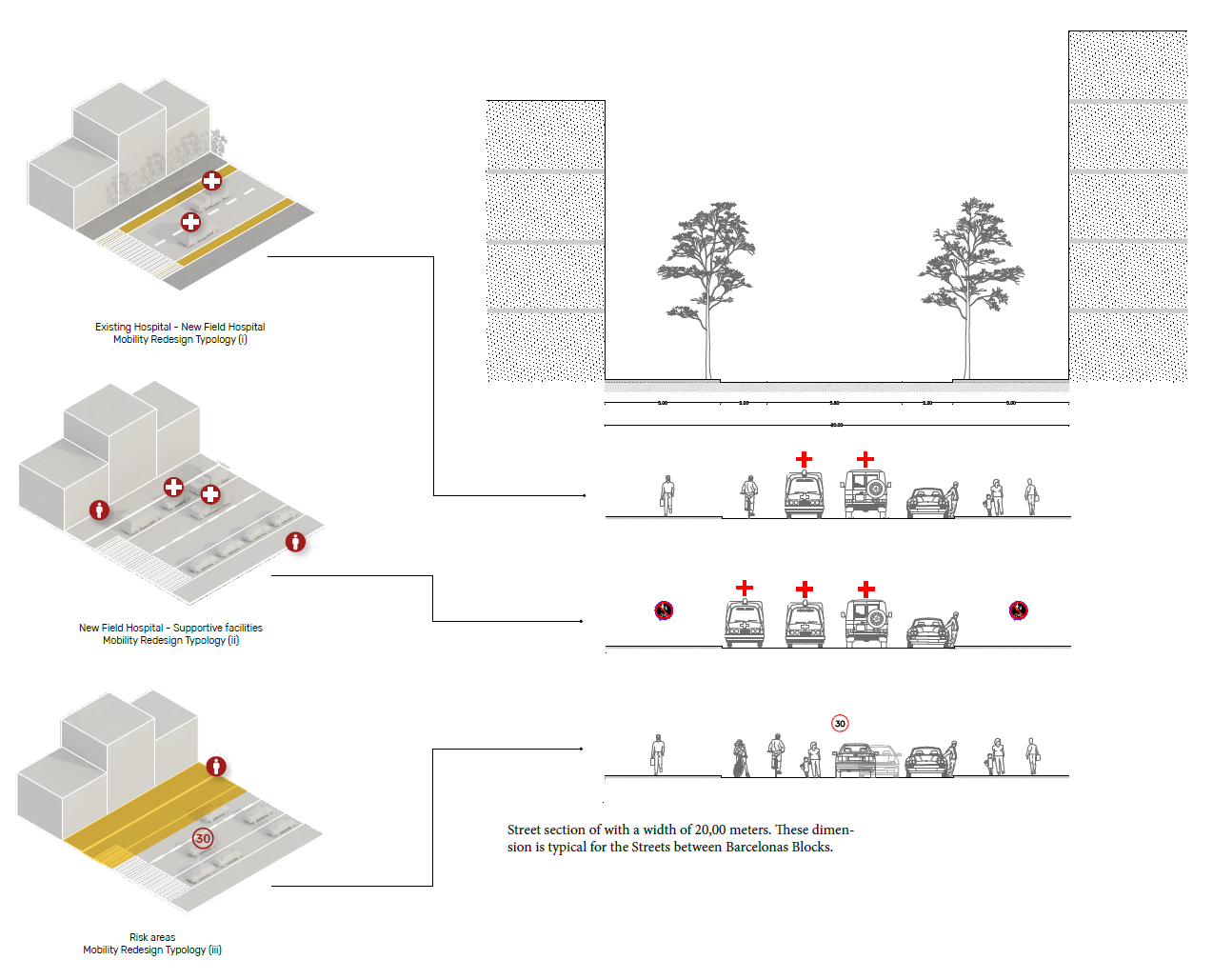
Reprogramming Mobility
Based on the Building Network, Streets will be redesigned to support the medical supply and safe People outside and inside the Building Network.
Private cars are not anymore dominating the streets so space can be redesigned to give prioritization the medical supply and patient transport but also outside the Building Network for pedestrians to support non-motorized mobility.
Credits
Reactive Pandemic Protocol is a project of IaaC, Institute for Advanced Architecture of Catalonia
developed at Master in City & Technology in (2019/2020) by:
Students: Jochen Morandell, Alejandro Quinto-Ferrandez, Rovianne Santiago
Faculties: Areti Markopoulou, Alex Mademochoritis, Iacopo Neri